
Difficult Case Types: Part 2, A Discussion of Adult Short-Term Orthodontics
Clear or Invisible braces for adults.
Originally posted on Dentistry Today.
INTRODUCTION
In part 1 of this article, I discussed the evolution and rationale of short-term orthodontics (STO); and how it dovetails with aesthetic dentistry and other disciplines to provide treatment by one provider in a coordinated and timely manner. I briefly discussed issues involving treating patients who present with bruxism, patients who have unrealistic cosmetic demands or obsessive-compulsive disorder, and those personality types who wish to alter or control their treatment plan. Though STO is oriented toward the patient’s aesthetic chief complaint, we must still limit the patient’s involvement in the treatment planning and smile design to meet “real world” expectations.
At the initial consult, it is helpful to provide cosmetic orthodontic patients with before and after pictures of what they may expect, along with a list of what can and cannot be achieved. All common significant questions should be addressed on one’s Web site, in addition to a consultation photo book given to new patients before seating. Actual pictures of one’s own work can be a fair representation of what to expect, providing an honest and direct dialogue that can be very beneficial to both the patient and the provider.
The case types discussed in the second part of this article include interesting aspects of transfer cases, the judicious use of enamel reproximation, cases with particular retention needs, cases with temporomandibular disorders (TMD), large tongues, profile problems, and a complex multidisciplinary case. These difficult case types offer an opportunity to present pearls that can enhance treatment for both STO and conventional orthodontics alike. The greater focus and time per visit required for STO (I prefer one-hour visits) also bring greater reward and satisfaction for both the patient and the provider.
CASE TYPE IV: TRANSFER CASE WITH TIPPED POSTERIOR TEETH
While some believe that they can nonsurgically expand the dental arch through orthodontics in an adult patient, it has been proven that “expansion” (crown tipping in an adult) at past the age of 13 years is not significant, and it is prone to relapse.1Posterior crowns tip to the buccal without significant root translation resulting in an unaesthetic and unstable result also prone to gingival recession.
 |
 |
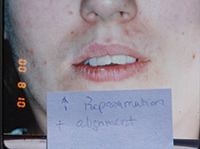
| Figure 1. Patient first came into our office with teeth tipped outward through use of removable expansion appliances. There was sufficient space for alignment, but the roots were in unstable positions with crowns tipped to the buckle. | Figure 2. A stable result must maintain arch circumference in an adult patient with the teeth in cortical bone to prevent inward collaspe post-treatment. |
 |
| Figure 3. Patient presented with narrow incisors due to previous treatment that relied too heavily upon enamel reproximation and scarificed tooth proportion and aesthetic outcome. |
Patient in Figure 1 was referred by an orthodontist in Los Angeles for lingual orthodontics. He expanded her for one year with Crozat appliances, leaving sufficient space to align the teeth (Figure 1). At this point, she moved to Boston, where we commenced lingual orthodontic treatment which proceeded smoothly. Brackets were removed with an aesthetic result. However, in the months after completion, the arch form and tooth roots continued to collapse inward. Expansion had spread the teeth laterally into an unstable position outside the cortical bone. The patient needed a brief course of retreatment with enamel reproximation which yielded a far more stable result which has been maintained well (Figure 2).
CASE TYPE V: OVERUSE OF ENAMEL REPROXIMATION
While the previous case showed an under-reliance on enamel reproximation, this case shows overreliance on it. Lack of flexibility and overreliance on any one treatment modality has its perils, though. The patient in Figure 3 was looking for retreatment despite the fact that her teeth were straight. In order to achieve an ideal occlusion nonextraction by the treating orthodontist, the teeth had been interproximally reduced to the point that they were unaesthetic, lacked embrasure space, and were not self-cleansing. This resulted in unaesthetic tooth proportions and perpetually inflamed papillae. Minor alignment was done along with recontouring. The teeth were shortened to establish better proportion, and embrasure spaces were opened to allow better self-cleansing.
CASE TYPE VI: SPECIAL RETENTION NEEDS; ADULT CLASS II, DIVISION 2; LARGE DIASTEMA, SEVERE ROTATION
The Class II, Division 2 is a common type of crowding where the upper centrals tip palatally and the laterals flare labially (Figure 4). Aesthetically conspicuous, it is usually a simple case to align dentally with enamel reproximation. These patients do not usually have a profile problem needing orthognathic surgery. As they are fully grown adult patients, skeletal change and complete overjet correction is not usually possible nonsurgically, so the upper central incisors will always tend to relapse palatally. Therefore, this is an ideal case for maxillary lingual splinting of teeth Nos. 7 to 10 or teeth Nos. 6 to 11. Slight overjet allows a durable splint to be placed out of occlusion in a case type that would otherwise be very prone to relapse. Recognizing the instability of cases that have a skeletal component is essential, and this patient’s aesthetics are basically identical today to the result (Figure 5), 12 years after completion, with no noticeable relapse due to her upper and lower lingual fiber-reinforced composite splints (Ribbond).
 |
 |
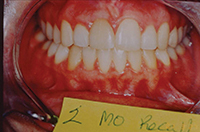
| Figure 4. Adult Class II, Division 2 is very prone to relapse. | Figure 5. Splinted result maintained well (at 12-year recall). |
 |
 |
| Figure 6. Large diastema needing fixed retention. | Figure 7. After short-term orthodontics (STO) with splinting. |
 |
 |
| Figure 8. The 3.5-year recall with fiber-reinforced composite (FRC) (Ribbond) splints. | Figure 9. Severely rotated incisor. |
 |
 |
| Figure 10. This rotation could never be maintained without a splint. | Figure 11. Four-year recall with maxillary FRC splint. |
Large diastema cases (Figures 6 to 8) also have special retention needs (a maxillary splint), as do severely twisted teeth (Figures 9 and 10). Though it requires overjet be left in the final result, the maxillary splint provides excellent retention, though it can require maintenance. Removable retainers would almost surely fail to retain these particular tooth movements. However, with the maxillary splint, the excellent results were well-retained in both cases at the 3- and 4-year recalls (Figures 8 and 11). Few orthodontists finish cases with the overjet needed to allow for placement of a maxillary splint.
CASE TYPE VII: Temporomandibular Disorder
This patient was a bruxer whose crowding and anterior recession were worsened by bruxing forward, causing anterior displacement of an upper central incisor (Figure 12). As a prominent cosmetic dentist, he came to Boston for rapid cosmetic orthodontics. The alignment proceeded smoothly with one exception: I allowed the likable dentist-colleague to limit my enamel reproximation in the lower arch. Therefore, my ability to retract the lower incisors and establish sufficient overjet also became limited. Parafunction usually ceases at the beginning of orthodontic treatment, but then returns once the teeth are no longer sore. Once the parafunctional bruxing returned, the upper central (that now had been retracted back) caused a more retrusive and limiting anterior guidance on the mandible (Figure 13). The new incisal guidance brought less freedom of the mandible during bruxing, pushing it backward, so disc compression and tinnitus followed.
 |
 |
| Figure 12. Bruxer, before STO, with protruded tooth No. 8 from bruxism. | Figure 13. Bruxer, after STO, with normal incisor occlusion. |
Our typical treatment method of leaving overjet avoids any retrusive incisor contact on the mandible, and avoids TMD sequelae. The lack of tight anterior coupling in my finished orthodontic cases accounts for the fact that I rarely see TMD in my patients after STO—a remarkable statistic, especially considering occlusal change is not the primary treatment focus. One must be very cautious when leaving a case with the incisors tightly coupled together in occlusion, as any lower incisor relapse or change in jaw position forward may cause disc compression and the pain that may or may not have been poresent beforehand.
CASE TYPE VIII: LARGE TONGUE
Patients with a large tongue often have anterior spacing. The patient’s tongue in Figure 14 already fills the space available and goes to the lingual surfaces of the teeth. While the anterior spacing can be reallocated distal to the canines, the incisors cannot be retracted and maintained inside the neutral zone with long-term stability. The tongue pressure will push the teeth forward unless tongue reduction has occurred. In such cases, we always explain to our patients at the initial consult that space will be redistributed distally to maintain an incisor position that is in harmony with the tongue, instead of a retracted incisor position when the tongue will not allow them to be maintained and would cause relaspe.
CASE TYPE IX: PROTRUSION WITH UNAESTHETIC PROFILE
There is no STO solution for cases with an unaesthetic facial profile and lip incompetence. This case needed bicuspid extraction because the amount of upper incisor retraction required cannot be done with enamel reproximation alone (Figures 15 and 16).
 |
 |
| Figure 14. Large tongue prohibited the retraction of incisors. | Figure 15. Bicuspid extraction case with lip incompetence. |
 |
 |
| Figure 16. After bicuspid extraction treatment. | Figure 17. Surgical case that requires a referral to the surgeon-specialist team. |
 |
 |
| Figure 18. Canine substitution needed for missing upper lateral incisors. | Figure 19. Final result; bonded and splinted upper canines and bicuspids without any bridgework or implants. |
Even more involved, the skeletal case in Figure 17 clearly needs orthognathic surgery.
CASE TYPE X: MULTIDISCIPLINARY CASE
This case cannot be done with orthodontics alone (Figures 18 and 19). Treatment involved surgical exposure and bringing down impacted canines throughout one year (still considered STO due to the complexity of the case), as well as splinting with reshaping and bonding. Canine substitution was done for the missing upper laterals incisors. With some creative thinking, this patient avoided any bridgework or implants as this result was achieved solely with orthodontics and bonding. Most patients enjoy a result with greater simplicity, stability, and predictability, while eliminating implant surgery and minimizing treatment time and expense. This type of thinking can bring people back to dentistry, especially adult patients like this with aesthetic problems who have not sought out care sooner due to obstacles inherent in a conventional and more involved treatment plan. Patients opt out of 2-year treatment when there is a shorter plan with proven results.
CONCLUSION
As dentists, we have a myriad of responsibilities that can make dentistry complex as well as rewarding. Diagnosis and treatment planning, patient management, and retention protocol all vary with a need to understand and accommodate each patient’s teeth and character. Comprehensive 2-year orthodontics may better address more complex cases, but there is also a demand for more rapid orthodontic treatment for the typical adult cosmetic cases.
We must always remember that elective cosmetic dentistry of any type often comes with a human dimension of personal preferences that is often distinctive. These preferences must be understood, addressed, and ideally, satisfied, within the parameters of a healthy and stable long-term result.
Reference
- Bishara SE, Jakobsen JR, Treder J, et al. Arch width changes from 6 weeks to 45 years of age. Am J Orthod Dentofacial Orthop. 1997;111:401-409.