Six-Month Adult Aesthetic Orthodontic Treatment
Straight teeth in just six months.
Posted on Glidewell Laboratories.
While cosmetic dentistry has commanded more attention with recent breakthroughs — such as all-ceramic crowns, veneers, composite materials and intraoral cameras — the demand for adult cosmetic orthodontic treatment has also increased. It has been estimated that in 1970, only 5 percent of adults aged 18 or older sought consultations for comprehensive orthodontic treatment.1 In 1990, four times that number sought consultations for orthodontics.
Currently, adults present with chief complaints about the crowding of their teeth more frequently than anything else.2 Many adult patients want to straighten their teeth, but they are unwilling to wear braces for two or more years. Patients presenting with a physiologic occlusion and a desire for aesthetic improvement can benefit from orthodontic correction that requires only a short treatment time of six months or less. Adults who have their teeth straightened experience a better body self-image and higher self-esteem.3,4 The general public is focused on a noncrowded, aesthetic tooth arrangement more so than orthodontists, who are also concerned with occlusal and skeletal relations.5 A short, six-month treatment can very well enhance periodontal and occlusal aspects of the patient’s dentition. Treatment, therefore, serves as an adjunct to final periodontic and restorative treatment, even though the main focus remains cosmetic.
Simultaneously treatment planning the orthodontics with the cosmetics, crown & bridge, and periodontics in the same office facilitates a well-orchestrated cosmetic result, which can be more difficult to achieve through cross communicating between specialists. In this context, limited cosmetic orthodontic treatment is best done on patients who otherwise may not opt for comprehensive orthodontic treatment.
Method
The first aspect of case selection involves a discussion of the patient’s chief complaint. Patients are given a list of orthodontic and cosmetic problems, and asked to indicate their objective(s) for seeking treatment. In almost 90 percent of adult cases, relieving anterior crowding is the primary concern. This figure is based on 20 to 25 new orthodontic consults per month for six months in my general practice.
When the patient is committed to treatment, a database of information should be obtained: panoramic and full-mouth radiographs, intraoral and extraoral photographs, and models. A problem list is then reviewed with the patient, followed by a comprehensive treatment plan. The orthodontic aspect should be cosmetically oriented, specifically excluding skeletal problems. Because the profile and posterior occlusion are not to be changed significantly, a lateral cephalometric X-ray is not necessary.6
The treatment sequence includes the following:
- Data collection and records;
- Prophylaxis, fluoride application, oral hygiene instruction, and endodontic and periodontic disease resolution;
- Extraction of third molars and a lower incisor when necessary (other teeth may rarely need to be extracted);
- Cosmetic orthodontics; and
- Bleaching, crowns and cosmetic bonding when indicated
If the patient prefers not to wear Hawley retainers, teeth can be retained by splinting once settling has occurred.
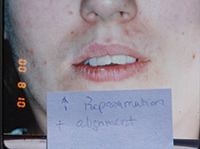
The Case for Enamel Reproximation
Because the postextraction health of the temporomandibular joint has been questioned, bicuspid extraction is now done with less frequency than in the past. It provides a result that is not always aesthetic or stable, has been slowly decreasing in popularity (almost 8 percent between 1988 and 1993), and remains controversial, varying widely among practitioners.7-10 Almost one and a half years is required to close the extraction spaces, and nonextraction patients have fuller lip support following treatment.11 Expansion is also a questionable method of treatment because long-term stability is doubtful.12
However, enamel reproximation allows for minimal localized tooth movements, fewer extractions, maintenance of lip support and shorter treatment time. Begg theorized that crowding of most dentitions is actually the result of decreased proximal wear, which our evolutionary predecessors once experienced.13 Therefore, enamel reproximation would seem to be the most natural available remedy for relieving crowding.
Enamel reproximation (air-rotor stripping) can be done for up to a 10 mm arch-length discrepancy. Sheridan recommends limiting reproximation to 1 mm per contact or 0.5 mm per proximal surface.14,15 Frequently, more than this can be done without noticeable change in tooth morphology or sensitivity because it’s done throughout six months in conjunction with fluoride treatments. It has also been theorized that the resultant flat interproximal contacts may actually increase post-treatment stability.16 Anterior lower arch crowding greater than 4 mm should be treated with the extraction of a lower incisor, followed by reproximation to minimize the black triangular space at the gumline. In most cases, a space determination is performed by resetting the teeth on the models with wax to measure the space required. This also allows a preview of the aesthetic result for both patient and doctor.
Appliances
Brackets should be bonded to the first molars using a straight-wire technique and NiTi wires. Posterior brackets with a larger (0.022) bracket slot placed in an ideal, aligned position minimize posterior occlusal changes. Successive reproximation using double-sided fine diamond discs (Brasseler) is followed by the use of fluted carbide burs for finishing and rounding enamel edges. Interproximal over-reduction can rarely cause transient tooth sensitivity.
All teeth should be gradually aligned with local reproximation, progressively heavier wires and chain elastics. The principal tooth movements include rotations, tipping and vertical movements as opposed to translation and root torquing. By minimizing root movement and bone remodeling, treatment time is decreased. Profile change, relapse and root blunting are also minimized, which is significant because root blunting can occur when moving roots greater distances throughout a longer period.
Retainer wear is recommended for six months (full time), six months (at night) and three nights per week until stability is achieved. Post-treatment fiberotomies should be performed for all rotations. Following two months of retainer wear to allow for occlusal settling, cosmetic alterations may be performed, such as cosmetic bonding, bleaching, all-ceramic crowns, enamelplasty and gingivectomies. Teeth deficient in a mesial-distal dimension (peg laterals, enamel erosions or broken teeth) should be built up before treatment to allow for proper final tooth positioning.
Case I
The patient presented with typical Class I crowding with aesthetics as the chief complaint. Rather than expand the arches into an unstable position prone to relapse in the adult patient, or reproximate lower incisors so much that they impinge on the gingival embrasures, it was decided to remove a lower incisor. The uppers were reproximated using a Brassler diamond disc and edges recontoured. The treatment was seven months and the patient was splinted afterward. Some molar supra-eruption occurred because of an anterior composite bite plane that relieved the deep bite and decreased the likelihood of further attrition in the anteriors.
Case II
The patient was referred by a local dentist who had done simple orthodontics, but who was not willing to treat occlusal problems. The patient had crowding with a bilateral crossbite that was causing both anterior and posterior attrition at a young age, requiring orthodontics.
The crossbite was corrected through the use of cross-arch elastics from the lingual of the upper molars and bicuspids to the buccal of the lowers. Enamel reproximation made space to treat the anterior crowding. Upper and lower bonded Ribbond splints served to reinforce the bonded incisal areas caused by attrition. It also provided resistance to fracture, as the splints produce a greater bonded surface area and composite thickness. An upper posterior Hawley retainer prevented relapse of the posterior crossbite.
Case III
This patient presented with the chief complaint of a large diastema. She had advice from numerous orthodontists who expressed different opinions regarding how to correct this (because of her deep bite and lack of lower spacing), as well as reservations regarding the possibility of successful retention. At our consultation, it was explained to the patient that our plan would include:
- Upper and lower anterior retraction and possibly lower enamel reproximation because of extra space on the uppers;
- A fixed composite bite plane on #8 and #9 lingual to relieve the deep bite by causing posterior supra-eruption;
- Possibly redistributing excess space to the distal of the upper canines to limit the retraction required; and
- An upper splint, which would be required. Removable retention is unacceptable in these cases. Therefore slight overjet in the final result is planned to make space for the splint.
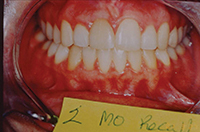
Per usual protocol, a prophy, bitewings, panoramic X-rays and restorative work were completed first. The patient’s treatment lasted five and a half months, with splinting and bleaching occurring on the final visit. At recall, the patient’s Ribbond splints were intact as she was not a bruxer. It is unlikely that this case would have succeeded without fixed retention.
It has been estimated that in 1970, only 5 percent of adults aged 18 or older sought consultations for comprehensive orthodontic treatment. In 1990, four times that number sought consultations for orthodontics.

Conclusion
Six-month adult cosmetic orthodontic treatment has a 60 percent acceptance rate among new patient consults in my practice, and post-treatment satisfaction is high. Many adults who undergo treatment have previously declined comprehensive treatment in other offices. Enamel reproximation, extraction of a lower incisor for space and limited occlusal change are among the modalities making this treatment unique and well accepted by patients. Offering clear or lingual appliances increases the patient’s cosmetic options. Treatment planning the orthodontic and restorative phases together facilitates patient understanding and communication, and delivers an outstanding cosmetic service. Patients with TMD, skeletal chief complaints, severe over/underjet, occlusal problems or very deviated midlines may opt for comprehensive treatment by an orthodontist. However, for the majority of adult patients with simply unaesthetic, crowded, spaced, functionally efficient and non-TMD dentitions, dentists should focus on the aesthetic chief complaint by performing conservative attenuated treatment in the general practice.
References
- Gottlieb EL. 1990 JCO study of orthodontic diagnosis and treatment procedures: results and trends. J Clin Orthod. 1991;24:145-56.
- Nattrass C, Sandy JR. Adult orthodontics—a review. Br J Orthod. 1995 Nov;22(4):331-7.
- Varela M, García-Camba JE. Impact of orthodontics on the psychologic profile of adult patients: a prospective study. Am J Orthod Denofacial Orthop. 1995 Aug;108(2):142-8.
- Lew KK. Attitudes and perceptions of adults towards orthodontic treatment in an Asian community. Community Dent Oral Epidemiol. 1993 Feb;21(1):31-5.
- Cochrane SM, Cunningham SJ, Hunt NP. Perceptions of facial appearance by orthodontists and the general public. J Clin Orthod. 1997 Mar;31(3):164-8.
- Proffit WR. Contemporary orthodontics. 2nd ed. St Louis: Mosby; 1993. p. 155.
- Little RM, Riedel RA, Engst ED. Serial extraction of first premolars—postretention evaluation of stability and relapse. Angle Orthod. 1990 Winter;60(4):255-62.
- McReynolds DC, Little RM. Mandibular second premolar extraction—postretention evaluation of stability and relapse. Angle Orthod. 1991 Summer;61(2):133-44.
- Weintraub JA, Vig PS, Brown C, Kowalski CJ. The prevalence of orthodontic extractions. Am J Orthod Dentofacial Orthop. 1989 Dec;96(6):462-6.
- O’Connor BM. Contemporary trends in orthodontic practice: a national survey. Am J Orthod Dentofacial Orthop. 1993 Feb;103(2):163-70.
- Paquette DE, Beattie JR, Johnston LE Jr. A long-term comparison of nonextraction and premolar extraction edgewise therapy in “borderline” Class II patients. Am J Orthod Dentofacial Orthop. 1992 Jul;102(1):1-14.
- Glenn G, Sinclair PM, Alexander RG. Nonextraction orthodontic therapy: posttreatment dental and skeletal stability. Am J Orthod Dentofacial Orthop. 1987 Oct;92(4):321-8.
- Begg PR. Stone Age man’s dentition. Am J Orthod. 1954;40:298-312.
- Sheridan JJ, Ledoux PM. Air-rotor stripping and proximal sealants. An SEM evaluation. J Clin Orthod. 1989 Dec;23(12):790-4.
- Sheridan JJ. The physiologic rationale for air-rotor stripping. J Clin Orthod. 1997;31:609-12.
- Peck H, Peck S. An index for assessing tooth shape deviations as applied to the mandibular incisors. Am J Orthod. 1972 Apr;61(4):384-401.
 Dr. Georgaklis is an expert in dentistry. He combines orthodontic techniques with cosmetic practices to give you a straight smile. And the best part about his work? It’s done in just six months! No case is too difficult for Dr. G. — 90% of his patients get straight teeth in six months or less.
Dr. Georgaklis is an expert in dentistry. He combines orthodontic techniques with cosmetic practices to give you a straight smile. And the best part about his work? It’s done in just six months! No case is too difficult for Dr. G. — 90% of his patients get straight teeth in six months or less.